Paper Source Data Is Costing Your Trial 6 Months: The Case for eSource
In clinical research, source data is the original recording of information used to reconstruct and evaluate a trial. When that source is paper, every downstream step involves manual transcription, physical transport, and human verification. Each step introduces delay and error. eSource, the direct electronic capture of data at the point of care, eliminates the entire chain.
The real cost of paper
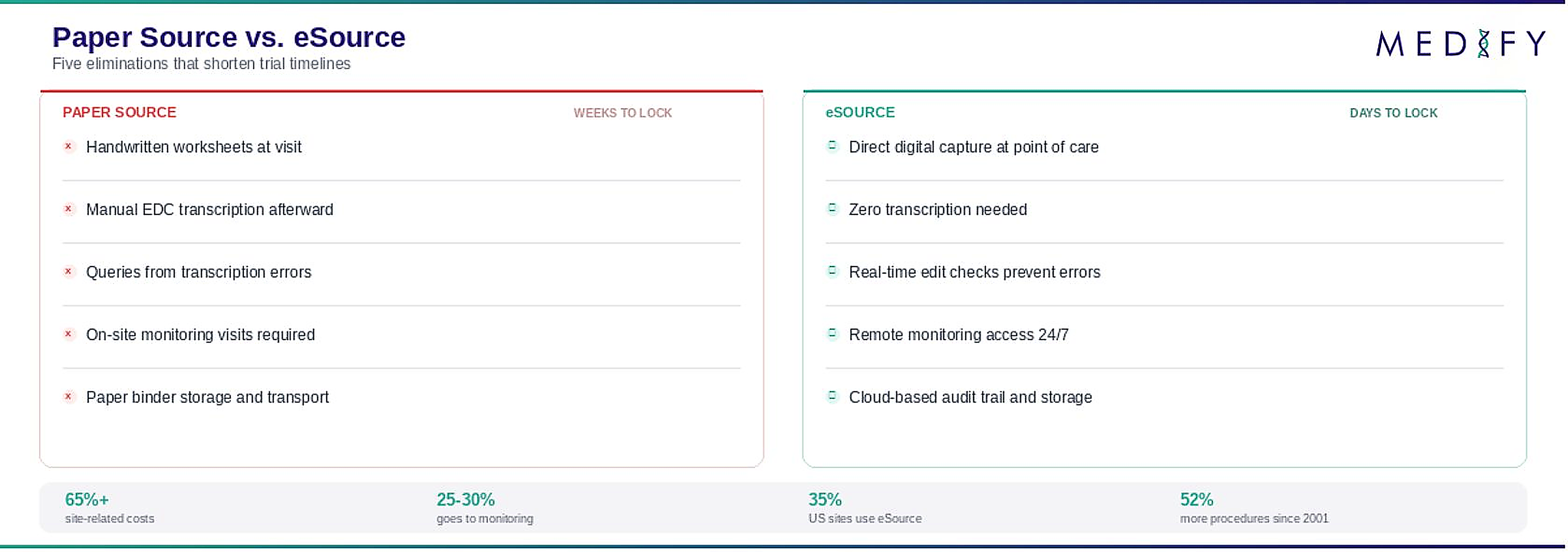
The cost of conducting biomedical research has increased exponentially over the past six decades while net productivity has declined. More than 65% of total clinical trial costs are site-related, covering site management and trial work where protocol-mandated activities have escalated in complexity.[1]
A significant portion of this cost comes from the transcription workflow. In a paper-source trial, coordinators record data on printed worksheets during patient visits, then manually enter that data into the sponsor's EDC system afterward. This double data entry consumes time and introduces transcription errors.
Monitoring alone accounts for approximately 25 to 30 percent of total trial costs, with on-site source data verification being a major contributor. Much of this cost exists specifically because paper source data cannot be reviewed remotely.[2]
Where paper costs compound
What the data shows
A comparative effectiveness study published in JAMIA tested the hypothesis that eSource data management reduces time and transcription errors. Using time-and-motion methods with direct observation by industrial engineers, the study confirmed that eSource was associated with a significant reduction in both data entry time and data quality errors.[1]
A separate ACRP study examined the effect of eSource on protocol deviation rates across three independent study sites transitioning from paper. The findings were clear: eSource reduced the incidence of protocol deviations compared to paper source.[3]
ICH-GCP E6(R3) and the regulatory push
The revised ICH-GCP E6(R3) guidelines explicitly encourage the use of digital systems to improve trial execution. The revision acknowledged a 52% increase in unique procedures in Phases I through III and a 48% increase in cost per patient visit between 2001 and 2015.[4]
eSource aligns directly with R3 principles. It enforces ALCOA-C data entry standards with built-in audit trails and access controls. It supports quality-by-design through predefined data fields and logic checks.[5]
The FDA has been equally explicit. Their guidance on electronic source data states that it promotes capturing source data in electronic form to streamline and modernize clinical investigations.[6]
The adoption trajectory
An estimated 35% of US-based research sites have adopted site-based eSource systems, with adoption especially concentrated among higher-performing professional sites. On some Phase 3 trials, more than 50% of US sites now use eSource.[7]
In Central and Eastern Europe, adoption is significantly lower. Most CEE sites still operate on paper source, creating a growing gap between the data quality expectations of global sponsors and the operational reality at regional sites.
What eSource eliminates and what we've seen
The practical impact is five eliminations: transcription errors disappear because data is entered once at the source. Storage costs disappear because there are no paper binders. Transport delays disappear because data is available instantly. Retrospective monitoring disappears because real-time access enables continuous oversight. Manual compliance documentation disappears because the system generates it automatically.
In our own pilot work, we've observed the effect directly. When site coordinators capture data electronically at the point of care instead of transcribing from worksheets afterward, the time from patient visit to clean data record drops from days to minutes. Queries that previously arose from illegible handwriting or transposition errors stop occurring entirely. The data is cleaner not because people are more careful, but because the system prevents errors at the point of entry.
The bottom line
Paper source data is a legacy workflow that persists not because it works well, but because it is familiar. The research is unambiguous: eSource reduces errors, reduces deviations, reduces time, and reduces cost.
For clinical research organizations in Central and Eastern Europe, the transition from paper to eSource is not a technology upgrade. It is an operational survival decision.
References
- [1]Kush RD, et al. JAMIA, 2018. PMC5942198
- [2]RealTime eClinical. "What is eSource in Clinical Trials?" Feb 2024.
- [3]Andrus J, et al. ACRP, April 2023. acrpnet.org
- [4]Getz KA, et al. TIRS, 2024. doi:10.1007/s43441-024-00671-0
- [5]Cosmos Clinical. "eSource in Clinical Trials." Sep 2025.
- [6]FDA. "Electronic Source Data in Clinical Investigations."
- [7]CRIO. "eSource vs. EDC." Aug 2025. clinicalresearch.io
This article is part of our Insights series on clinical trial technology in Central and Eastern Europe.
About Medify. Medify is an integrated ePRO, eSource, and data collection platform purpose-built for clinical trials in Central and Eastern Europe. Deployable in 4 to 6 weeks with ICH-GCP E6(R3) and GDPR alignment. medifyclinical.com.